


A study published yesterday in the British medical journal The Lancet examining the effectiveness of antidepressant medication in children and teens is receiving lots of attention on the internet and is worthy of comment.
A group of scientists, led by Dr. Andrea Ciprani of the University of Oxford (and funded by the Chinese government) analyzed the results of 34 randomized clinical trials of antidepressant medication used specifically to treat major depression in the pediatric population. These are not new studies, but this is a new interpretation of older results by combining many studies addressing the same issue. Here's what they found, gently edited for lay readers...
We deemed 34 trials eligible, including 5260 participants and 14 antidepressant treatments. The quality of evidence was rated as very low in most comparisons. For efficacy, only fluoxetine was statistically significantly more effective than placebo. In terms of tolerability, fluoxetine was also better than duloxetine and imipramine. Patients given imipramine, venlafaxine, and duloxetine had more discontinuations due to adverse events than did those given placebo.
When considering the risk–benefit profile of antidepressants in the acute treatment of major depressive disorder, these drugs do not seem to offer a clear advantage for children and adolescents. Fluoxetine is probably the best option to consider when a pharmacological treatment is indicated.
Something for parents, families, pastors and other church leaders to consider when kids are suspected to have depression and in need of help is that within the professional and mental health support communities, perceptions about the effectiveness of antidepressant medication in kids is very different from the clinical reality suggested by the research literature.
The vast majority of clinical trials of antidepressant medication for the treatment of depression in children and teens have failed to demonstrate a statistically significant difference between the response to medication vs. placebo pills. We used to think that kids responded differently to antidepressants than adults because of developmental differences in the activity of neurotransmitters, such as serotonin. It turns out there’s little difference between the response of these medications in adults to what we see in kids and teens. To explore this further, allow me to introduce you to the concept of effect size.
When a pharmaceutical company submits a drug to the FDA for marketing approval, they’re required to demonstrate in two separate clinical trials that the drug is better than nothing (placebo). As a clinician, I want to know how much better than nothing the drug is for the condition I’m seeking to treat. That’s where effect size comes in.
Effect size is a measure of the magnitude of the difference between the change from baseline seen with an active treatment compared to the change from baseline seen with placebo. Without going into the formula for calculating effect size (beyond the scope of this post), we usually end up with a ratio ranging from zero to one. When an effect size is below 0.20, the benefit of the treatment to an outside observer would be essentially imperceptible. An effect size of 0.50 suggests a moderate effect. Effect sizes of 0.80 and above suggest a robust effect. For the sake of comparison, here are some examples of effect sizes of treatments for ADHD:
- Diets restricting artificial dyes and preservatives: 0.19
- Omega-3 fatty acid supplementation: 0.36
- Atomoxetine (Strattera): 0.60
- Methylphenidate-based stimulants (Concerta, Focalin): 0.80
- Amphetamine-based stimulants (Adderall, Adderall XR, Vyvanse): 0.93
Check out the illustration below...This data is taken from an independent review commissioned by the FDA of all the placebo-controlled trials of serotonin reuptake inhibitors (SSRIs) and other second-generation antidepressants in children and teens. SSRIs are the most commonly used antidepressants...Prozac, Zoloft, Celexa, Lexapro, Paxil and Luvox are SSRIs:
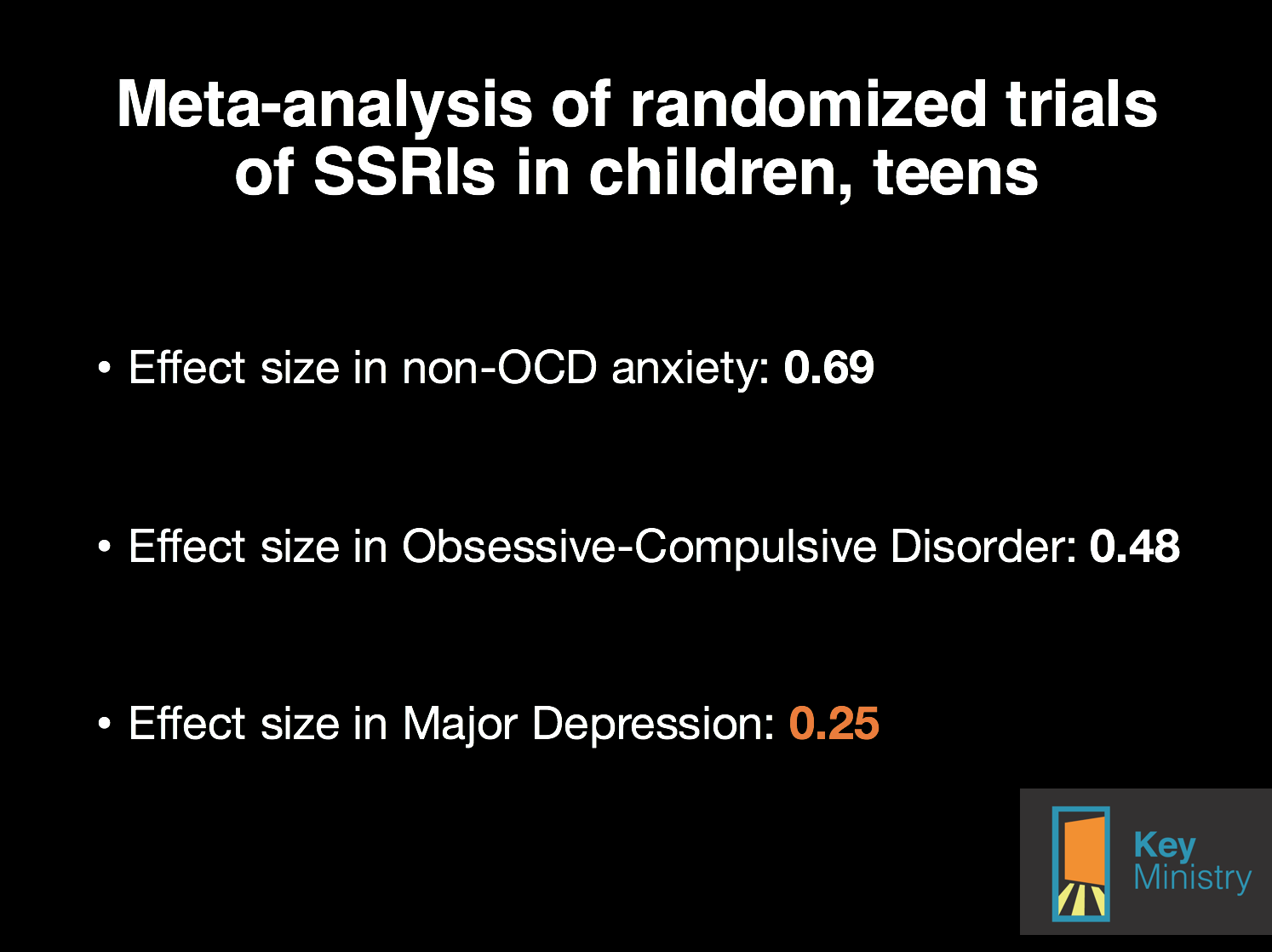
Source: Bridge JA et al. JAMA 2007; 297(15) 1683-1696
It turns out that the antidepressants are reasonably effective anti-anxiety treatments in children and teens. SSRIs are moderately effective for Obsessive-Compulsive Disorder. The effect size of SSRIs for treating depression is relatively small.
Another way of looking at this issue is by considering another statistical concept, the number needed to treat (NNT). The NNT represents the average number of patients one would need to treat to be assured a positive response was due to the effect of medication as opposed to placebo. The NNT for antidepressants in kids when used to treat depression is 10. For OCD, the NNT is 6. For other anxiety disorders, the NNT is 3.
Here's the meta-analysis of the research literature on antidepressants in adults authored by Dr. John Ioannidis. Quoting from the paper:
The meta-analysts found 74 eligible FDA-registered trials with 12,564 patients. Among them, a third (n = 26 trials [31%] with 3449 patients) had remained unpublished. The FDA had determined that half of the registered trials (38/74) had found statistically significant benefits for the antidepressant ("positive" trials). All but one of these trials had been published in journals. Conversely, of the other half trials (36/74) that were deemed to be "negative" by the FDA, one in three were published as "negative" results; another 11 trials were published, but the results were presented in such a way so as to seem "positive" and 22 "negative" trials were silenced and never appeared in the literature.
The meta-analysts studied the estimated effectiveness of these drugs when data were combined from the FDA records and when data were combined from the published literature. For all drugs, the published literature inflated the effect sizes. The inflation varied from 11% to 69% and it was 32% on average. The FDA data would suggest that these agents had small, modest benefits (standardized effect size [ES] = 0.31 on average). Conversely, for 4 of the 12 agents, if one were to perform unawares only a meta-analysis of the published data, the summary result would suggest clinically important effectiveness (ES>0.5). This was not true for any agent based on more complete FDA data.
Here are a couple of thoughts to consider...
The professional community, parents and families hold assumptions about the effectiveness of psychotropic medication, especially medication for depression, that are unrealistic based upon our understanding of the research literature.
It's very possible (I'd argue it's very likely) that adults and children who respond positively to antidepressants do so not because they're experiencing a placebo response, but because we're treating anxiety symptoms that frequently predispose, precipitate and perpetuate feelings of depression.
*****************************************************************************************************************
Key for Families has launched our first seven Facebook communities for families of kids with disabilities. We have communities for...

- Adoption and Foster Care
- Autism and Asperger's Disorder
- Homeschooling parents
- Mental health
- Ministry families
- Parents of adult children
- PTSD and trauma
Key for Families Facebook communities are free, but registration is required. Sign up for one or more communities today, and share the invitation with friends who might want to join.

