


In this talk from Disability and the Church 2023, Dr. Steve Grcevich discussed topics and trends he observes in the medical and mental health professions likely to impact the disability ministry community and shared ideas for how the individual Christians and the Church as a whole might prepare to serve the vulnerable in the months and years to come. He urges followers of our ministry to share with anyone who might be encouraged or inspired by his message.
For those of you who follow our ministry, you know that I haven’t been nearly as visible as a few years ago. My work as a child and adolescent psychiatrist has left me very tired, very burned out, and very angry. The mental fatigue from all the clerical and administrative tasks involved with helping families access the support services and medication they need has made it more difficult for me to exercise the emotional self-regulation expected of a ministry leader and elder in the church.
One conclusion I’ve come to with the help of a trusted friend and ministry coach is that I need to accelerate the process of “retiring” from medicine to ministry for my own spiritual well-being and the sake of my witness to others. With that said, I’ve come to recognize much of my anger may represent a sort of “holy discontent.” My ministry coach suggested I consider how the trends I’m observing in medicine and the struggles I see in kids and families served by my practice might inform and impact the ministry done by churches supported by Key Ministry.
For the most part, I’ve loved being a physician for the last 37 years. While I’ve primarily been a clinician, I’ve had a hand in research that’s helped lots of kids and families and helped to inform our ministry. As a med school professor, I’m involved with one of the most important areas of our curriculum - teaching the principles of evidence-based medicine.
I’m occasionally asked how I reconcile my faith with my roles as a physician, scientist and child psychiatrist. That’s never been a problem, because there’s a common thread that connects my roles - the pursuit of truth.
Jesus refers to himself as the Way, the Truth and the Life. The pursuit of truth inevitably leads us to Christ. While most of my colleagues don’t share my faith, we historically shared a mutual desire to pursue the truth of how our bodies and brains work. The process of discovering truth often included some vigorous arguments based upon our research and our observations, but the end result was usually a better understanding of how to serve the kids and families in our care.
Not anymore. There’s stuff we can’t talk about. I’m angry, embarrassed and ashamed by what has become of my profession. The pursuit of truth that historically characterized medicine is rapidly taking a back seat to the embrace of an “anti-culture” within our large healthcare institutions, our professional societies and medical schools characterized by unquestioning affirmation of expressive individualism and radical self-determination. An ethos in which identity is substantially based upon sexual preferences and a subjective, internal sense of gender and understood in the context of systems of oppression rooted in Western culture. The antipathy toward Western culture in our profession is antipathy to the Christianity foundational to Western culture. The anti-culture is a rejection of the idea that our identity as humans is that of embodied beings created in the image of God, a rejection of the natural law evident in the created order that provides even those who don’t know or acknowledge God with a sense of right and wrong. The anti-culture is a rejection of the created order, and by extension, a rejection of the Creator Himself.
My profession of medicine is at the forefront of a movement that increasingly seeks to pervert God’s created order. Confusing kids about what it means to have been created as male or female. Distorting marriage and usurping the family structure established from the time of creation – the God-given structure for raising children foundational for our civilization. Twisting language in such a way that words lose their meaning. Killing preborn children is “reproductive health care.” “Pregnant persons. “Men” who menstruate.
We have a word to describe efforts to twist and distort the creation God described as good. We don’t use it very often – but I think it’s appropriate here. That word is evil.
In Ephesians 4:26, the Apostle Paul encourages us to “be angry and not sin” – implying anger is a normal, human condition that’s not sinful when we deal with it appropriately. In the next chapter (Ephesians 5:11) he tells us “Take no part in the unfruitful works of darkness, but instead expose them” and at the end of Romans (Romans 12:21) he implores us to “not be overcome by evil but overcome evil with good.”
I’ve been wrestling a lot with what will look like for however long I continue to serve in medicine and for the work I do through Key Ministry. And I’ve been angry at myself and disappointed in myself for the excuses I’ve made for not confronting practices in my field that are just flat out wrong.
What makes you angry in a way that compels you to overcome evil with good? I’d guess if you’re here this weekend, you’re angry when you see disabilities get in the way of individuals and families coming to know Christ, serving and being served through the local church. How are you called to overcome evil with good where God has placed you? And do you have the courage to do something about it?
The Christian church gained influence within the Roman culture in the first, second and third centuries because of the love and concern individual Christians demonstrated for the most vulnerable in society. Our predecessors in the faith adopted the children who were abandoned and unwanted, many because of illness or disability. Their courage was on display when they risked their lives by staying behind in the cities caring for the sick through the plagues that regularly ravaged the population. Their values were foundational to our healthcare system, much of which in America was established by Christians and Christian denominations.
The disability community in America will soon confront the reality of a medical community engaged not just in preserving life, but in ending life. I got a call last month from a staff person with the Christian Medical Dental Association looking for physicians willing to testify before a state legislature in the Northeast against granting the “right” to physician-assisted suicide to college-age adults whose capacity for higher-order thinking and decision-making hasn’t yet fully developed.

On the other side of our church’s baptistry across the street, physician-assisted suicide is now the sixth leading cause of death in Canada. Canada has “temporarily” put on hold plans to expand the right to physician-assisted suicide to individuals with primary mental health conditions and to “mature minors.” The College of Physicians and Surgeons in Ontario has declared that the refusal to provide an “effective referral” to a willing colleague if a physician is unwilling to kill a patient who meets criteria is an ethical violation that justifies taking away that physician’s license to practice medicine. And it is killing. In 99% of cases, the physician or medical practitioner personally administers the lethal dose of medication. In debate on expanding the right to suicide to minors, a pediatrician from the college recently argued that parents be given the right to request their child’s physician to administer lethal doses of medication to infants up to age one born with “severe malformations,” “grave and severe illnesses” or infants whose “prospective of survival is null, so to speak.”

Increasingly, reports are coming out of Canada of persons with disabilities seeking out physician-assisted suicide because of difficulty accessing necessary healthcare services or appropriate housing and support. In some instances, healthcare professionals are reportedly suggesting suicide as a solution to their suffering. The U.S. is five to seven years behind Canada in expanding access to “medical assistance in dying.” Ten states now have physician-assisted suicide provisions, and legislation has been introduced in ten additional states.
The medical ethicist Dr. Farr Curlin has described the emergence of a “Provider of Services” model within medicine in which patient autonomy is paramount, and physicians are expected to support patients’ decisions so long as they are legal and technologically feasible. In this model, a physician’s conscientious objection to a procedure that a patient desires violates the very aim of the medical profession. Patients have the right to choose the services they believe contribute to their well-being and physicians are obligated to accommodate patients’ choices, even when those choices conflict with the physician’s conscience or ethics.
We’re fortunate in Ohio that our legislature approved a “right of conscience” law stipulating that professionals in our state can’t lose their licenses for refusing to participate in treatments or procedures that violate their religious beliefs. I find it unsettling that the lobbying in OPPOSITION to the law was led by the Ohio State Medical Association, the Ohio Academy of Family Physicians and the Ohio Hospital Association.
Another trend I find infuriating is the way in our medical societies justify their social cause of the moment by claiming their cause of the moment for is “evidence based,” even when the evidence basis is limited is to non-existent. Who can forget our public health officials who boldly asserted that the dangers of COVID necessitated the closure of our schools and churches, but protests in support of social causes they supported justified the risks? Or the church that moved worship services to a casino in a state where casinos were open but churches were closed?
When the U.S. Supreme Court overturned Roe v Wade, my professional society issued a policy statement - “To ensure the healthy physical, mental, and developmental health of children and adolescents, the American Academy of Child and Adolescent Psychiatry recommends ensuring children and adolescents have access to evidence-based reproductive health services, including abortion. I’m convinced our professional societies make these pronouncements with the assumption no one with the ability to call them out on falsehoods could possibly disagree with them. I did a literature search of the National Library of Medicine after receiving that e-mail. There is NO evidence abortion has mental health benefits for adolescents. The more appropriate question based upon the research is the extent of psychological harm experienced by teens who undergo the procedure.

The most conspicuous misuse of the term “evidence-based” involves the claims of the American Academy of Pediatrics and the Endocrine Society regarding interventions they describe as “gender affirming care” in children and youth. The British Health Service shut down their nation’s gender medicine clinic after a comprehensive review of the research on the services provided there to children and teens, concluding “Evidence on the appropriate management of children and young people with gender incongruence and dysphoria is inconclusive both nationally and internationally.”

Why talk about “gender-affirming care” at a disability conference? The disability scandal nobody’s talking about is the vulnerability of kids with preexisting mental health conditions or developmental disabilities to gender ideology. When the British government shut down the Tavistock Center, the London clinic that exclusively provided gender-affirming care to kids throughout the U.K., 35% of kids treated through the center were identified with moderate to severe autism – seventeen times the reported rate of autism in the nation at the time.
A couple of months ago, I was sitting at the kitchen table of a family I’ve known for a long time. Their son on the high end of the autism spectrum has struggled with social isolation and social anxiety for a long time. His parents were thrilled when he finally found a peer group at school. Except that every kid in his new circle of friends is a girl who thinks they’re a boy and lunchtime conversations center on how they might persuade their parents to take them to the gender clinic at the local children’s hospital. My patient has now become resolute that he's really a girl. I won’t forget for a long time the fear on his mother’s face as her son and I spoke and the tenacity with which he clung to this newly acquired perspective was evident. This is a fear often expressed by parents of my patients on the high end of the spectrum in the privacy of their appointments.
I can remember one lecture of the hundreds I sat through during my general psychiatry residency at the Clinic in the late 80’s. The Grand Rounds speaker was discussing approaches to kids born with ambiguous genitalia or abnormalities of sex-linked chromosomes. The takeaway was that the worst thing you could do to a kid was cause them to experience confusion over gender.
The embrace of the gender revolution by the medical establishment and our academic institutions is the ultimate gaslighting. If they, with the support of the media and our internet overlords can convince the public that a person with male genitalia and a Y-chromosome in every cell in their body is a female, there is no lie our culture shapers won’t be able to propagate.
I’ve always taken it as a given that an important part of my job as a child psychiatrist is to promote healthy reality testing. Affirming distorted gender identity is antithetical to everything I was trained to do. I learned early on you don’t affirm delusional thoughts that are out of touch with reality. If I’m asked to see a young person with psychosis who thinks they’re Jesus, I don’t bow down to them and call them “messiah.” We don’t agree with teens with anorexia who insist they’re too fat or tell kids with body dysmorphic disorder they’ll be happier and look great after they get the plastic surgery they want. My profession has literally shot its’ credibility to hell and violated a trust that won’t be repaired for a long time, if ever.
So…what do we do as church, and how should the disability ministry movement lead the church when the caregivers and institutions persons with disabilities depend upon reject the Imago Dei?
1. Our most effective and impactful witness to the people in positions of influence in medicine, education and people of a similar mindset and worldview who shape the larger culture is the love we demonstrate through our care of the most vulnerable in society. Folks in my line of work are more likely to see the Bible as a tool of oppression than a repository of truth. What DOES get their attention is when they see us providing respite care for families of kids with disabilities who can’t access respite anywhere else, providing foster families for kids who have experienced serious trauma and neglect, helping the uninsured or underinsured access necessary medicine, medical equipment or services, or providing opportunities to persons with intellectual or developmental disabilities for productive and meaningful work and authentic community. Disability ministry is our most powerful witness to a hostile culture because it causes outsiders to reconsider the assumptions they hold about Christians and Christianity and disability ministry is a demonstration the church acting with integrity in however much of the Gospel they’re familiar with.
Are you angry about the diminished influence of the church in the culture and among our culture shapers? Start or grow a disability ministry. Start a mental health ministry. Support the families caring for kids who have experienced severe trauma.
2. We need to embrace a cradle-to-grave pro-life ethos. If you look at the trends Western culture regarding physician-administered suicide, persons with disabilities unable to access medical care, support services or appropriate housing are increasingly being offered death to obtain relief from their suffering. The church has appropriately demonstrated care and concern for women with unplanned pregnancies by establishing crisis pregnancy centers. If your church is in one of the ten states that currently permit physician-assisted suicide, or one of the ten states considering physician-assisted suicide it, think about what a “disability support center” might look like where those with conditions that qualify them for physician-assisted suicide might obtain the care, support and hope they need to bear their suffering.
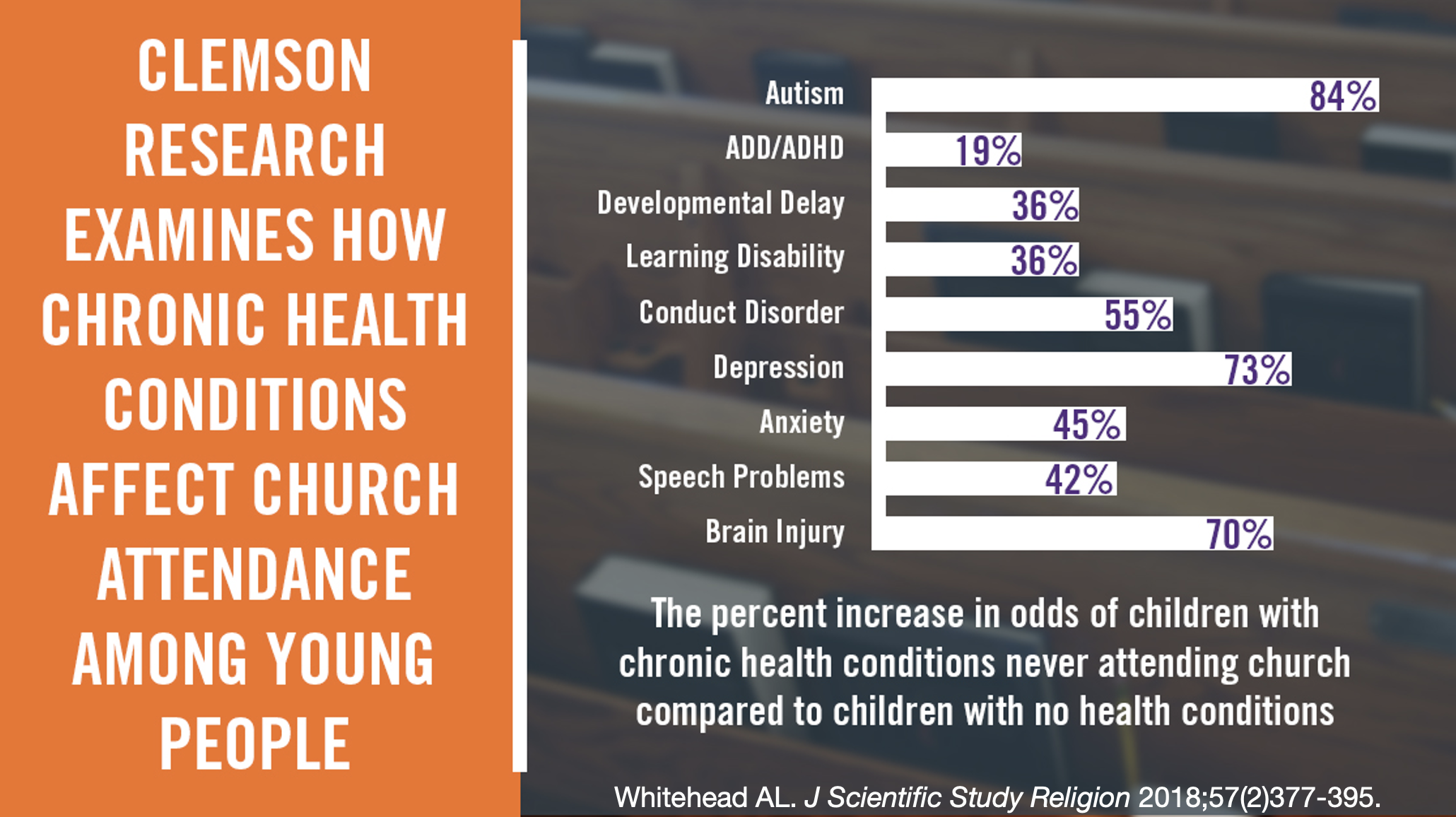
3. We need to do everything possible to promote mental wellness among the people of the church and our friends and neighbors not yet part of the church. I want to share this slide I’ve used in previous examining the impact of disability on family church attendance. We know that in absolute numbers, mental health disabilities, more so than any category of disability interferes with church attendance. While correlation doesn’t represent causation, I doubt it’s a coincidence that as mental illness becomes more common, church attendance is becoming less common.
We have some pretty good working hypotheses to explain the explosion of mental illness in recent years. We know the images and information our kids are bombarded with through their smart phones and social media apps contributes to increased rates of anxiety and depression. We know more people are more socially isolated than ever before. Part of why society is in the situation we’re in is that in supporting the autonomy and freedom and personal choice necessary to support and sustain the sexual revolution, we’ve embraced a moral relativism that requires us to kick aside the God-given guardrails regarding sexuality, gender, and marriage we need to thrive. The breakdown of the traditional family structure is producing an epidemic of trauma. Experience of trauma greatly increases the risk of mental illness, and people with mental illness who have experienced trauma often fail to respond as well to our traditional treatments.
The culture we’re living in is toxic to our kids. If they’re going to make it through with their mental and emotional health, but far more importantly, if they’re going to make it through with their faith, we need to create a counterculture in which they’re surrounded by peers raised with the same beliefs by parents in relationship with other Christian parents committed to raising kids with a Biblical worldview through which they might make sense of what the world tosses at them and acquire the confidence to overcome it.
Our counterculture is going to be built around strong churches and strong Christian schools. Why should parents of kids with disabilities have to use public schools to get the specialized education and supports their kids need? Christian schools should represent the model our public schools emulate. Our next front in the disability ministry movement needs to be mental health inclusion and inclusion in Christian schools and universities.
4. We need individual Christians to demonstrate courage in the face of extraordinary pressure to conform to defend the vulnerable when our medical and mental health professions have abandoned their moral compasses and act at odds with their historic purposes.
Most of my colleagues working in large healthcare institutions or academia recognize that to speak out against this is likely to be career-ending. The medical profession has become a reflection of a culture that silences those with approaches or ideas that challenge those in positions of authority.
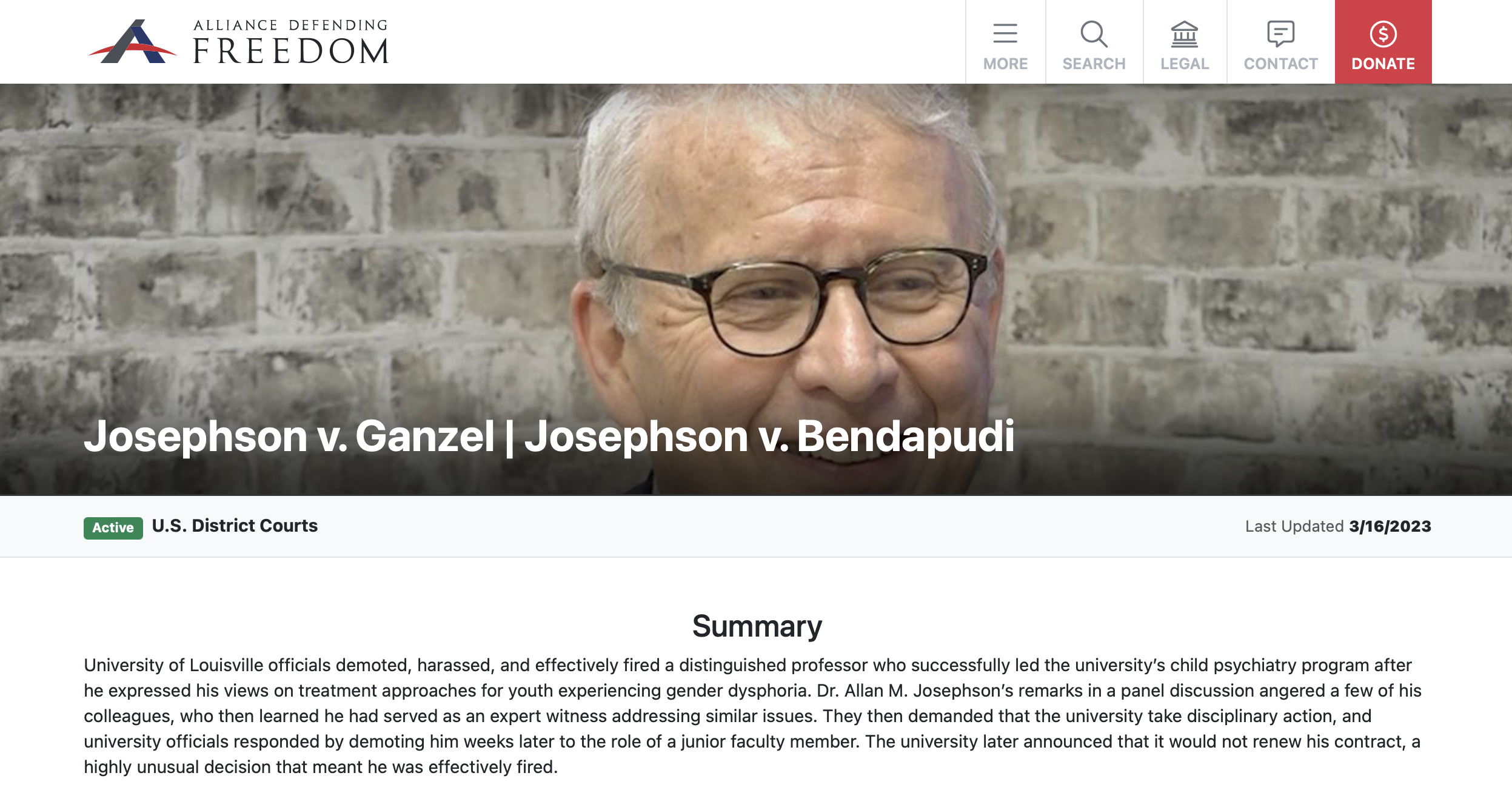
I want to tell you about a colleague of mine. This is Dr. Allen Josephson. He’s a child psychiatrist who built the department at the University of Louisville. We met working on stuff for the American Academy of Child and Adolescent Psychiatry’s Annual Meeting. He served as the head of the psychiatry section of the Christian Medical Dental Association. And he’s been unemployed for the last five years. He was fired by his university after speaking at an event in Washington where he advocated for supportive therapy as opposed to puberty blockers or hormones for kids struggling with gender discordance. The Alliance Defending Freedom accepted his case and is representing him as his case proceeds through Federal Court.
This is hard. Several years ago, one of our ministry volunteers in a position to do very impactful public advocacy asked me to get involved in speaking out against common treatment practices in pediatric gender medicine. I came up with all kinds of reasons to say no. I’m not an expert. I need to make a living. I don’t want our ministry to become a target for the activists and government officials bought into these agendas. I’m embarrassed and ashamed by my response.
Part of our job description as Christians is to witness to the truth and care for the vulnerable – and kids with autism or kids with mental health conditions who latch onto gender as an explanation for their discomfort in their bodies or parents who are emotionally blackmailed into consenting to unproven treatments by gender clinic staff with unsubstantiated claims their children will kill themselves if denied access to those treatments – I’m pretty sure they qualify as “vulnerable.“
I’ve reached out to some colleagues in recent weeks to see if they might be willing to advocate publicly on these topics. All of them responded as I did three years ago.
I’d like to say a few things publicly that need to be said by someone in my profession with my background and experience. Somebody needs to go first. My hope is it will be easier for others to speak if they know they’re not alone.
Children do best when they’re raised in homes with a mother and a father who love one another, serve one another, sacrifice for one another and are mutually committed for life to one another in marriage.
Medical interventions intended to end human life don’t constitute “health care.”
No one is “born in the wrong body” - and pretending that someone is of the other sex when the DNA in every cell of their body says otherwise is a lie and represents a disservice to the person who is person who is suffering.
I’ve experienced stuff in my practice over the last few years that make me – an evangelical Presbyterian – wonder if this is what spiritual warfare is like? And at the risk of sounding like someone who should be talking to somebody like me, I wonder if what “cancel culture” is truly about is canceling the Gospel?
It’s no accident that you’re here this weekend. God has obviously put something upon your heart to minister with folks with disabilities. I hope He’s given you lots of new resources and relationships to accomplish that work this weekend. Where do you sense God’s calling you to be courageous? Where is he calling you to take some risks that may make you very uncomfortable? To say some difficult or uncomfortable things?
Is he wanting you to start a respite care ministry through your church? Expand your ministry offerings for kids on the high end of the spectrum in need of healthy peers? Taking in a foster child with behavioral challenges? Helping families find counselors who are thoughtful and conservative in their approach with kids who struggle with self-image and identity? Advocating before your local school board, hospital board or state legislature? Or simply speaking the truth in love and encouraging others to do the same?
I’d like us to leave here this weekend with the courage to do the hard and uncomfortable things the Holy Spirit nudges us to do and committed to encourage and support one another through the struggles. Our team at Key Ministry is honored we get to do ministry with all of you and privileged to support you in any way we can.

