


The following is the prepared text for a talk by Dr. Grcevich offered in a symposium on the youth mental health crisis through the Gospel Initiative at Denver Seminary in Littleton, CO on February 9th, 2024.
I’d like to thank Jason and Dr. Young for inviting me to be part of this symposium today offered under the banner of the Gospel Project. I’m honored to be (in all likelihood) the first child psychiatrist invited to speak at Denver Seminary.
I love the learning objectives that you created for this conference. I’ve had a unique opportunity for the last nine years to contribute segments on youth mental health to the morning drive-time talk show on our Moody Radio affiliate in Cleveland. Two weeks ago, the show’s producer asked me if I could find something positive to talk about for a change. The show’s host, Brian Dahlen used your conference objectives as his talking points and we wrestled with the questions you posed.
I’m incredibly encouraged to be here today. You can’t imagine how alone I feel nowadays seeing to advocate for kids with mental health issues within my profession and within the church. Many days I find myself identifying with Elijah when he was on the run from Jezebel, thinking he was the only one honoring God through his ministry. I’m grateful your presence at the conference proves I’m not alone.
In our time together, I’d like us to focus on the most important manifestation of the youth mental health crisis that the church needs to address, share a number of ideas for how local churches and individual Christians might care for and support the kids and families affected and consider what leaders within the institutions and ministries of the “Big C” church might do to promote the movement beginning to sprout to address the needs of kids and adults in our culture struggling with mental health issues.
I’ll begin with an aspect of the mental health crisis that I almost never hear discussed. It should be the most important aspect of the crisis to pastors and other church leaders, and it’s the issue that drives the work done by our team at Key Ministry.
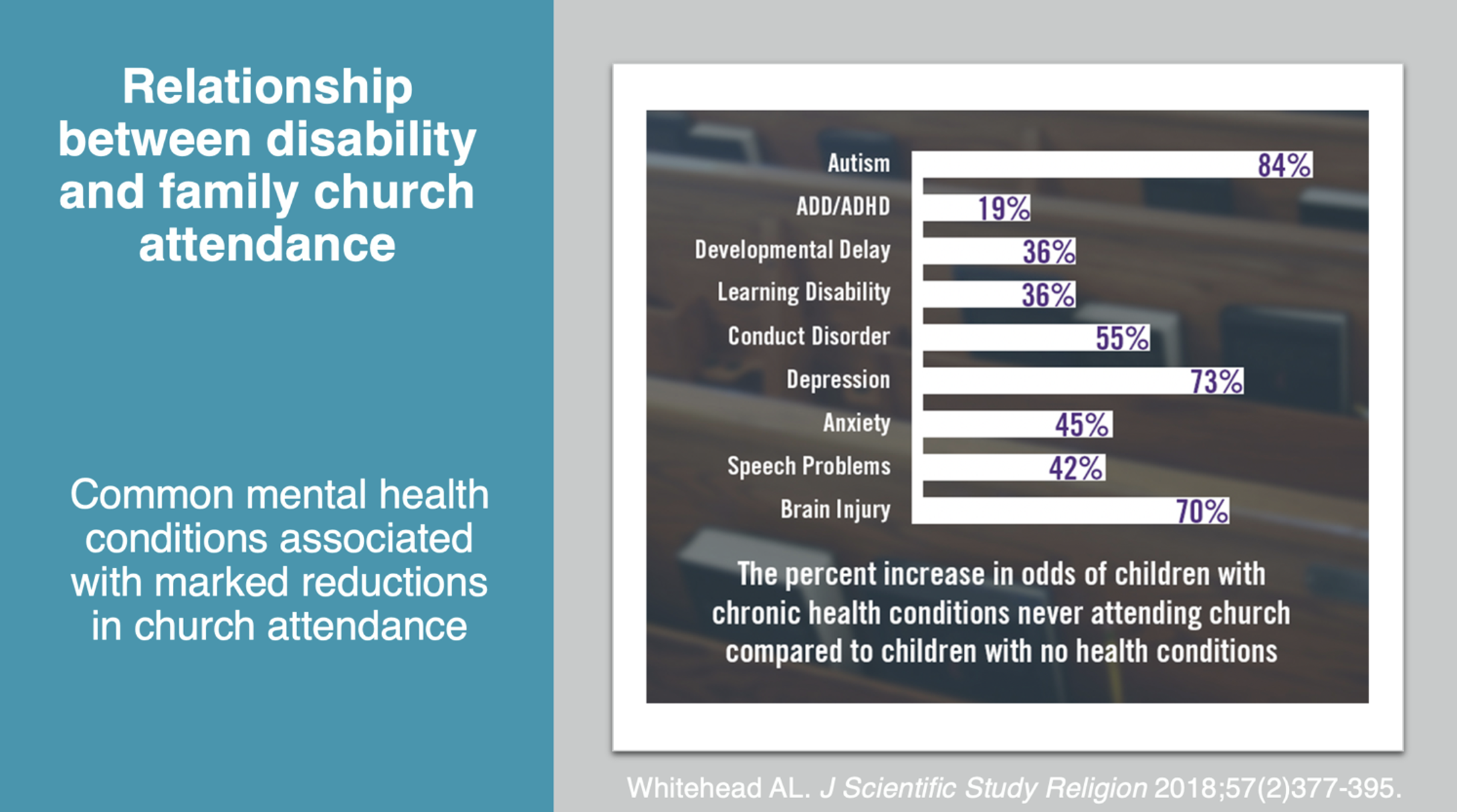
The disability community in general, and specifically families impacted by mental illness may represent one of the most underserved populations by the North American church. This study, published by Andrew Whitehead examined the relationship between the presence of a child in the home with a medical, mental health and developmental disability and family church attendance, using data from over 250,000 interviews conducted in three successive waves of the National Children’s Health Survey.
To no one’s surprise in disability ministry, the presence in the home of a child with autism decreases the likelihood of that child’s family setting foot in a church in any given year by 84%. But the presence of a child with depression is associated with a 73% decrease. Disruptive behavior disorders - Oppositional Defiant Disorder or Conduct Disorder results in a 55% decrease. Anxiety disorders - the most common mental health condition seen in adolescents - produces a 45% decrease. The presence of a child with ADD or ADHD decreases the likelihood of a family attending church at least once a year by nearly 20%. The 84% figure reported for families of kids with autism is a product of the comorbid mental health conditions most kids with autism experience.
20% of school-age kids in the U.S are identified with one or more significant mental health conditions. But this phenomenon of mental health issues and family church attendance impacts more than 20% of the school-age and adolescent populations. These kids with mental health concerns have parents, siblings and caregivers who don’t get to hear the Bible teaching, fellowship, and support that comes from being part of a caring church community, and their absence deprives us of their God-given gifts and talents intended to strengthen the body of Christ during a challenging time.
My breakout later in the morning will examine the obstacles that interfere with church attendance and assimilation and present the framework for an outreach and inclusion strategy for youth with mental health issues and their families, but I’ll briefly introduce our model here.

The inclusion model is grounded in a cultural model of disability. When I refer to church culture, I’m describing our attitudes and beliefs regarding mental illness and our expectations for how people will act - and interact when we gather for worship, fellowship, Christian education or acts of service. Attributes (or traits) associated with common mental health conditions - intense anxiety in unfamiliar situations, unrealistic perceptions of how others experience us, executive function deficits manifesting as difficulties with self-control or self-regulating emotions, weaknesses in processing social cues, sensory processing differences that affect their experiences in the physical spaces where ministry occurs, social isolation that reduces the likelihood of having friends, neighbors or coworkers to invite them to church, combined with negative experiences of church that are often multigenerational in nature and the widespread perception that children and adults with mental health challenges aren’t welcome at church. In the breakout, I’ll present an overview of seven broad strategies churches can implement to minimize barriers to attendance and engagement.
The mental health crisis among our youth certainly fits under the umbrella of our Great Commission mandate. The way we come around these kids and their families to provide care, support and community is central to our Gospel witness. But we can’t lose sight of addressing their greatest need – a saving faith in Jesus Christ.
As we ponder the actions through which we seek to communicate Christ’s love to these kids and their families, we might begin by considering the factors contributing to the youth mental health crisis, and research on factors that promote positive mental health. Because my training as a physician was focused on identifying and solving problems, I’ll start there, with emphasis on the challenges the church and our other Christian institutions are in a favored position to address:
Technology/unfettered access to information - research on the impact of smartphones and social media has been extensively documented. The reality is that kids who don’t have access to the technology are at an extreme disadvantage when it comes to making and keeping friends. Our families need a community that will support them in modeling responsible use of technology.
Coping strategies modeled by adults - This was a huge issue during COVID and continues to be an issue. Kids learn how to process feelings of anxiety and how to deal with adversity by modeling the responses of adults in their lives.
Social isolation – Addressing social isolation should be a slam dunk for us. I can’t tell you how often the kids I see (or their parents) tell me how desperate they are to have good friends. For kids who haven’t been actively pursuing a sport or extracurricular activity, finding a peer group can be exceptionally challenging. We need to become more capable of including kids who are less socially adept into our youth programming - and educate the church kids on the importance of being kind to kids who come across as quirky or marginalized at school.
School (academic demands, peer interactions) - School has always been a major stressor for kids. We historically see major variation in mental health service use associated with the school calendar. Peer conflicts and interactions are one factor, and difficulty meeting the academic demands for school are another, especially as educational achievement has become essential for future career success. The explosion in ADHD diagnoses we’ve witnessed among teen boys between 2000-2015 has largely been driven by the need to pound square pegs into round holes in school. We know kids who struggle to meet academic demands are significantly more likely to experience other mental health disorders, particularly anxiety and depression.
Christian education is one area where we have a major opportunity. Our Christian schools and universities ought to be the model public and secular learning institutions look to for successfully serving and including youth with mental health concerns. That necessitates they be part of this dialogue we’re initiating here today.
Consequences of the Sexual and Gender Revolutions - including the impact of family structure. A Biblical anthropology of gender and sexual expression may be especially impactful in suicide prevention among youth. One of the dirty little secrets you’ll NEVER hear mental health professionals discuss is the relationship between sexual activity and suicidal behavior. Data obtained from the 2015 National Youth Health Risk Survey indicated sexually active youth with the same or both sexes were twelve times more likely and male teens who were active sexually with females only were seven times more likely to receive medical attention from a doctor or nurse following a suicide attempt than same-age peers who had never been sexually active.
A sophisticated understanding of the mental health challenges experienced by our youth and a commitment to addressing their needs is an indispensible component of our Gospel witness. Gender and sexual expression are a wedge issue separating young people from the church. So much of the argument for encouraging young people in expressing their gender identity and living out their sexual orientation is based on the demonstrably false claim that their mental health will suffer unless their sexual behavior and new identities are fully affirmed and celebrated. We need to demonstrate we care more for their mental health than the champions of the sexual and gender revolution.
Trauma – Our understanding of the experiences of our most vulnerable youth gained from leaders in adoption and foster care ministry are arguably our areas of greatest competency in youth mental health as the “Big C” Church.
Examining for a moment at factors associated with positive mental health in youth, nearly all are enhanced by involvement in the church. Supporting and engaging kids in ministry in support of their peers may be a powerful component of the church’s response to the youth mental health crisis.
The church is no longer in a position of influence to divert the tidal wave of cultural change contributing to the mental health epidemic impacting our youth. But we can create healthier environments within our Christian subculture where we still have a measure of control. I’d like to conclude by considering what this looks like at the local church level and what it might look like for leaders with platforms within the church, the Christian institutions that shape our future leaders, our schools and our parachurch ministries to come together as part of a larger movement of God.

Let’s start with action steps the local church might take in response to the crisis…
Develop an outreach and inclusion strategy for welcoming families experiencing mental health challenges - those connected with the church and families in the surrounding community who are absent from church.
Talk about mental health issues from the pulpit - undoubtedly, there are families who are struggling with these issues in our churches. But because of the stigma that lingers in the church - especially those that have adhered to more traditional theology in matters of sexuality and gender - many families suffer in silence. A LifeWay study of family members of adults with serious mental illness reported the #1 request of those families was for their pastors to talk about mental health-related topics from the pulpit because in doing so they gave families permission to talk about their struggles in their small groups and interactions with fellow church members.
Referral assistance to culturally competent professionals and treatment facilities. In the LifeWay study, the greatest disconnect between the mental health support churches think they offer in terms of mental health support and the supports family report are available to them was the availability of referral lists. The lists need to include professionals and facilities serving children and teens and the people on these lists need to be vetted. The well-known Biblical counselor Brad Hambrick developed interview questions for pastors and church leaders to use upon meeting with mental health professionals so they can refer with confidence and prepare members for their experience.
“Casseroles” – Is the care and support available to families of children being treated for mental illness comparable to that offered for medical illness? Will families who would receive meals and pastoral support when a child is admitted to the hospital for surgery get them if their child is admitted to a psychiatric hospital following a suicide attempt?
Respite care: Families of kids with mental health issues often struggle to find childcare. The day-to-day struggles involved with parenting put great strains on marital relationships and reinforce the social isolation couples all too often experience. Two national ministries - Nathaniel’s Hope and 99 Balloons operate multistate church networks providing respite care for kids with intellectual and developmental disabilities. Many churches open respite to “typical” siblings, eliminating the stigma kids with mental health concerns experience attending respite events for kids with “special needs.”.
From a Biblical witness standpoint, this support is the single most head-turning thing churches can do to change perceptions of our faith among secular professionals. Making respite available flies smack in the face of the assumptions they make that Christians are uncaring or insensitive to the needs of vulnerable kids and their families. The willingness of 200 adults and teens in my church to give up a Friday evening to provide respite for families of 75 kids from the community gets their attention unlike anything else we might do to witness to our neighbors.
Foster care and adoption ministry: Kids with mental health concerns are disproportionately represented in foster care and among those available for adoption, in part because of the trauma they’ve experienced and because kids in these situations often inherit a strong biological predisposition toward mental illness from their biological parents. For a long time, I believed mental health ministry for would gain entry into the church on the coattails of foster and adoptive families, because their needs for mental health support are so great.
Education and support: Both Fresh Hope and Mental Health Grace Alliance offer Biblically based mental health support group models being in hundreds of churches in the U.S. and overseas. Both offer group models designed specifically for teens and their families. Marketing the availability of these groups to the surrounding community is a great way to connect with families outside of the church. Offering community education events on topics related to youth mental health marketed to the larger community serve the same purpose and demonstrate to impacted families they’ll be welcome at church.
We’re facing a great challenge and a great opportunity. I describe it as a “God thing” because the need is so great that none of us can solve it through our own abilities without the powerful involvement of the Holy Spirit. We’re experiencing a convergence of events suggesting the time has come for the church to address a mental health crisis we’ve ignored for too long.
In the aftermath of the “Great Dechurching,” leaders with influence may view outreach and evangelism as worthy of time and resources. The authors of that book present data suggesting mental health may be a contributing factor. Empty pews and empty seats create an urgency to act that may not have existed before.
Our system of caring for kids with mental health struggles is helplessly broken. We can’t train professionals fast enough to take care of the need that exists. We need to adopt prevention strategies, help kids to develop resilience and establish a subculture in which kids can thrive while the surrounding culture vehemently rejects the anthropology and ethics the church provided as a foundation to Western civilization.
The medical and mental health professions who have shaped our understanding of mental illness are rapidly losing credibility. The professionals have no answers for the crisis. Our treatments aren’t effective as advertised. Clinics where care is provided are run like assembly lines. My profession is rekindling the fear that had been subsiding among parents that their child’s pediatrician or therapist will undermine behind closed doors the beliefs and values they seek to convey to their children. My profession champions cultural sensitivity until we encounter families who have a different worldview. I’m utterly embarrassed and ashamed by my profession’s promotion of the gender revolution. I fear pediatricians and pediatric subspecialists may never regain the trust we once held as nations throughout Europe slam the brakes on “gender-affirming” care for lack of evidence supporting the safety and effectiveness of such treatment.
We need better experts to speak into these issues. Twenty years ago, Protestant Christians were underrepresented in psychiatry by a factor of thirty. It’s no doubt worse now. We need a few Christian hospitals to step up and create world-class training programs specifically for psychiatrists, who because of their medical and psychological training are uniquely qualified to lead the church’s response to these needs.
Considering how the church might impact the youth mental health crisis feels a little bit like being the dog who catches the car. Now what? I sense we’re in the early stages of a movement along the lines of the one shaping disability ministry. There are values foundational to that movement that will likely shape this one.
Where do we go from here?

Our first challenge is to help people called to this ministry become connected to and networked with one another. We need to help leaders and influencers become known across the “silos” that exist in the church. When I consider our ministry’s plan and my personal calling over the next 12-18 months, it’s to bring people together to help them become aware of the work being done, the resources that have been created and the fellow believers inspired with similar passion and vision. We’re planning to host a conference this fall to gather leaders serving in this space with the hopes of developing a common agenda across organizations for supporting churches in supporting the mental health of their parents and children.
We need to identify leaders with platforms within the institutions of our subculture – seminaries and Christian universities, Christian school, children’s family and student ministry, the Biblical and Christian counseling communities, foster care and adoption ministries – called to champion the cause and connect them with the people and resources necessary to create synergies and optimize their impact.
Our brothers and sisters in Christ need tools to help their friends and neighbors inside and outside of the church who are struggling. The church collectively withdrew from this mission field two or three generations ago because the founders of the mental health professions rejected the truth of the Gospel and embraced moral relativism, exchanging love for thy neighbor for love for thyself. Their ideas captured the culture. The culture’s rejection of God and the created order of His universe has left tens of millions of children, young people and adults broken and in need of hope. In an unimaginably rich country, they’re our generation’s orphans and our vulnerable. It’s an incomprehensible privilege and honor for us to be part of his plan to redeem them.
When I prayed about what would happen at this conference I prayed that other seminaries grounded in sound and time-honored theology will be inspired to host events similar to this one, and that upon my return to my hometown known for exceptionally bleak weather and its’ failure to ever play in, much less win a Super Bowl I’ll find e-mails in my box from leaders with influence from all segments of our evangelical subculture interested in conversations and connection. I also prayed that this conference would help fellow believers with a similar calling to find one another.
No seminary, no church, no pastor, no school, no child psychiatrist, no professional and no Christian ministry can solve this problem. But all of us can do demonstrate the love of Christ for kids and families impacted by mental illness inside and outside of our churches.

Our team at Key Ministry would be honored to come alongside you as you take the next steps. We’ve got lots of resources available on our website and Catherine Boyle, our mental health ministry director and I are available to help any church or ministry looking to do more.
Thanks again to the leadership of Denver Seminary for inviting me to be with you. I can’t wait to see how God will use today’s event as a catalyst for a movement that will be an authentic Gospel witness and a blessing for so many.
For more on the Gospel Initiative at Denver Seminary, click here.

