


This is the text of Dr. Steve Grcevich’s speech at the Colson Center National Conference in Arlington, TX on June 1, 2024. Thanks to the team at the Colson Center for inviting us to be part of such a fabulous event!
I can’t begin to describe how honored I am to have been invited to your conference. There are many people here whose work I’ve followed and admired for a long time. I’m like a journeyman baseball player who gets invited to the All-Star game and feels out of place in the locker room.
I’m especially honored to be at an event connected with the Colson family. Chuck’s daughter Emily and his grandson Max have had an immeasurable impact in the church through increasing awareness of individuals on the autism spectrum and their families. About ten years ago, Emily came to my church for a local ministry conference. We expected 50 people and over 300 showed up. That’s Emily praying for the volunteers providing respite care for families who came to hear her speak. That event became the inspiration for Disability and the Church, an event our ministry hosts that’s grown into the largest disability ministry conference in North America.
I wear a lot of different hats. I’ve been a physician for 38 years and in practice as a child and adolescent psychiatrist for 33. I don’t think I’ve ever felt as angry and ashamed of my profession as I have the past two days. I’d like to start by apologizing on behalf of my profession to Autumn and Tammy. Unfortunately, Christians and courage are in very short supply in my specialty these days. I used to be involved with research on the safety and effectiveness of medications commonly prescribed for kids and teens with mental health concerns. I’m also a medical school professor – I taught evidence-based medicine for eight years until the school found other faculty to take over my teaching when I made some videos for the Identity Project pointing out the lack of evidence for what’s referred to as “gender-affirming care” for kids.
I’m planning to retire from clinical practice next year to serve full-time as the President of Key Ministry. We work with churches to help connect them with families of kids with disabilities, with a special emphasis on “hidden disabilities” - emotional, behavioral, developmental or neurological conditions lacking visible physical symptoms. From that context, I’d like to share some ideas about how we might love our neighbors with disability in the culture we currently inhabit.
First and foremost, we can welcome them to our places of worship where they might encounter truth, come to faith, grow in faith, cultivate meaning and purpose and experience genuine community.
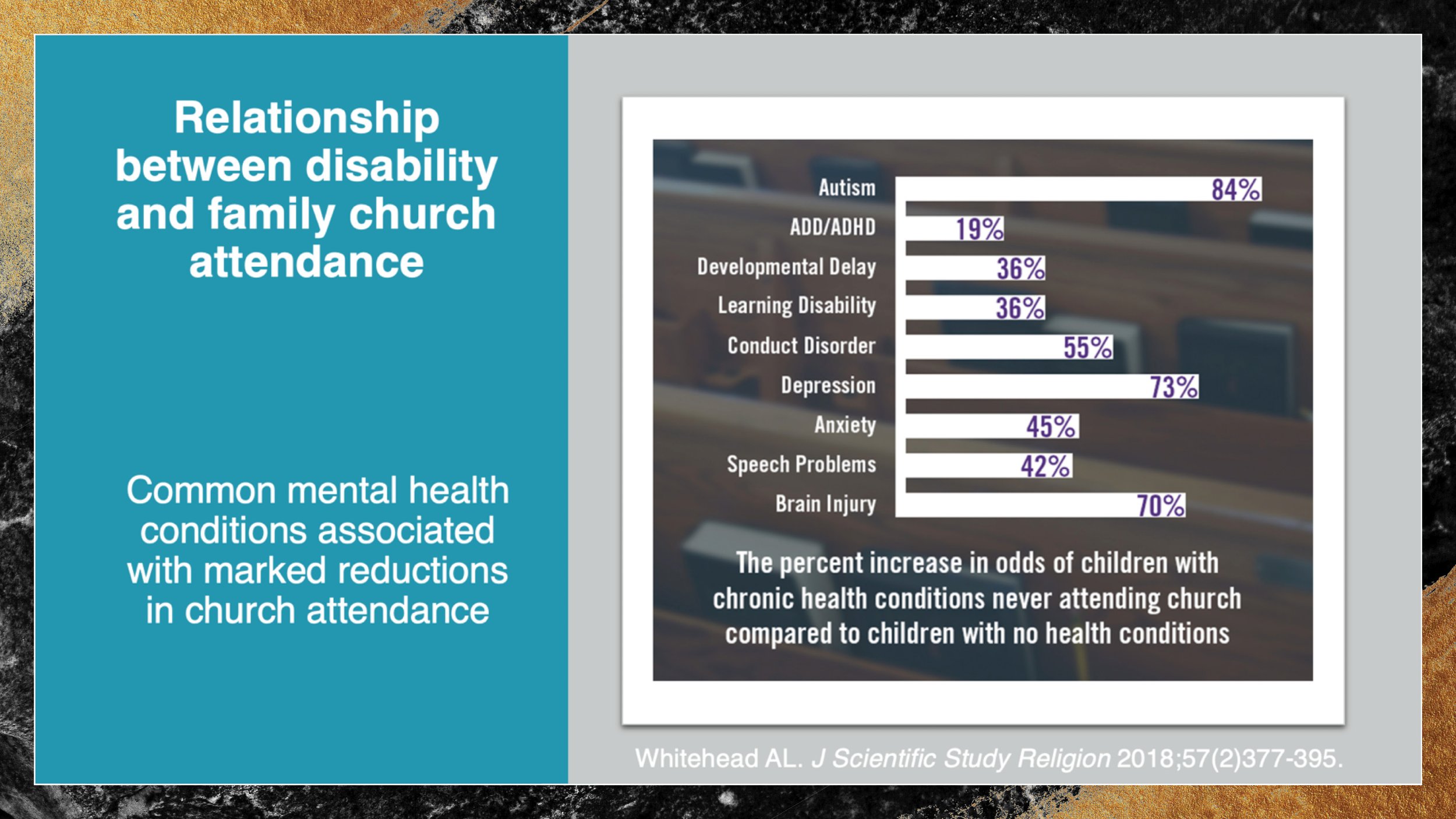
This 2018 study motivates the ministry I lead. Data from over a quarter million family interviews conducted in three successive waves of the National Children’s Health Survey were examined for the association between the presence of a child in the home with a disability and family church attendance. The presence of a child with autism decreases the likelihood of their family setting foot in a church by 84% Having a child with depression decreases church attendance by 73%. It’s 55% for families of children with disruptive behavior disorders - Oppositional Defiant Disorder and Conduct Disorder, 45% for families of kids with anxiety disorders and around 20% for families of kids with ADD or ADHD.
This is scandalous! Families impacted by disability represent arguably the largest underserved group by the church in North America.

Would you want Chuck Colson’s grandson and his family to be part of your church? This is Max Colson. He’s developed an incredible ministry - Hearts by Max - His artwork is used to create note cards for sharing words of encouragement. How many other families are there like Max’s who lack the opportunity to come to faith or live out their faith because they don’t have a church in their community prepared to welcome them? I’d hope that some of you here today will summon the courage after you get home to approach the leadership of the churches where you worship about the need to welcome families impacted by disability into your congregations. Our ministry team would be honored to prepare you for a conversation with your church leadership and provide them with all kinds of free training and support from our ministry or other like-minded ministries that serve alongside us.
Second, we can help our neighbors with disability by addressing heartfelt, but unmet needs. I’m convinced our most effective and impactful witness to the people in positions of influence in medicine, education and the larger culture is the love we demonstrate through our care of the most vulnerable in society. My professional colleagues are more likely to see the Bible as a tool of oppression than a repository of truth. When they see Christians providing respite care for families of kids with disabilities who can’t access respite anywhere else, opening their homes to foster kids who’ve experienced serious trauma and neglect or helping persons with intellectual or developmental disabilities to engage in productive and meaningful work – THAT they notice!
Disability ministry is arguably our most powerful witness to a hostile culture because it compels outsiders to rethink their assumptions about Christians and Christianity. It has power because it demonstrates the church acting with integrity with the portions of the Gospel outsiders may be familiar with..
We can work to ensure children and young adults with disabilities will have access to schools that teach from a Christian worldview and instill an understanding and appreciation of the Imago Dei. Young people growing up with disabilities need a sound understanding of the value our Creator places upon the bodies He has given us. There are lots of folks here serving in Christian education. Maybe your next step in exercising courageous faith is to advocate for inclusion of more students with special education or mental health needs into our Christian schools and universities? For far too long, Christian families have lacked alternative to public schools for the specialized instruction and therapies their kids need. Too many Christian schools have lacked the will to invest in the staff and supports necessary for kids with disabilities to attain their full potential. Our schools and universities should represent the model for supporting students with disabilities that our public education system seeks to emulate.
Finally – and it truly horrifies me to have to say this - if we’re serious about loving the most vulnerable among us we need to take bold steps NOW to protect children and adults with disabilities from the medical profession I’ve been a part of my entire adult life. The institutions that form the backbone of our profession have been captured by an ideology that worships radical self-determination, insists that future physicians understand their patients through a worldview categorizing them as victims or oppressors and see conscription into the sexual and gender revolution as a necessary condition for entry into the profession. The medical profession has recently made demonstration of proficiency in applying critical theory and intersectionality a requirement for graduation from med school and residency. You’ve heard all weekend about the evil creeping into our healthcare system. Children and adults with disabilities are far more dependent than others on an increasingly amoral system.
Dr. Cottle spoke about the MAID program in Canada. Believe it or not, a leading champion within Canada’s Parliament of the right to die for teens and persons with mental illness is Stan Kutcher, a child psychiatrist considered a world-class researcher in child and adolescent depression.
When I ran a large group practice, I banned the word “provider” in my office because I considered it demeaning. There’s a reason why that term has largely replaced the word “physician” in the healthcare system. Dr. Farr Curlin has described the emergence of a “Provider of Services” model in medicine in which patient autonomy is a paramount value and physicians are expected to support patients’ decisions so long as they are legal and technologically feasible. In this model, a physician voicing a conscientious objection to a procedure a patient desires violates the very aim of the medical profession. Physicians have moral agency, while “providers” do not.
Patients have the right to choose the services they believe contribute to their well-being and physicians are obligated to accommodate patients’ choices, even when those choices conflict with the physician’s conscience or ethics. This model has been fully embraced by the medical establishment. Several years ago, the legislature in my state wrote into law a “right of conscience” for licensed healthcare professionals. One of the most vocal opponents of conscience protections was the Ohio State Medical Association.
Medicine used to be a refuge for me from the political polarization that’s characterized our culture. I fear the leadership of our profession is losing the ability to view research objectively that doesn’t support their preferred political agendas. Lots of people are getting hurt as a result.
Our medical and professional societies in the U.S. refuse to acknowledge the actions of governments in the U.K., Finland, Sweden, Norway and France that are shutting down clinics providing “gender-affirming” care with kids because of the lack of evidence supporting the long-term safety or efficacy of these treatment approaches. My own professional society (AACAP) refused to allow a fellow child psychiatrist who oversees all treatment of youth with gender dysphoria in Finland to present an alternative perspective at our Annual Meeting.
The embrace of the gender revolution by the medical establishment and our academic institutions is the ultimate gaslighting. If they, with the support of the media and our internet overlords can convince the public that a person with male genitalia and a Y-chromosome in every cell in their body is a female, there is no lie our culture shapers won’t be able to propagate. In the process, we’re bringing about irreparable harm to countless children and adults while destroying the credibility of the medical profession.
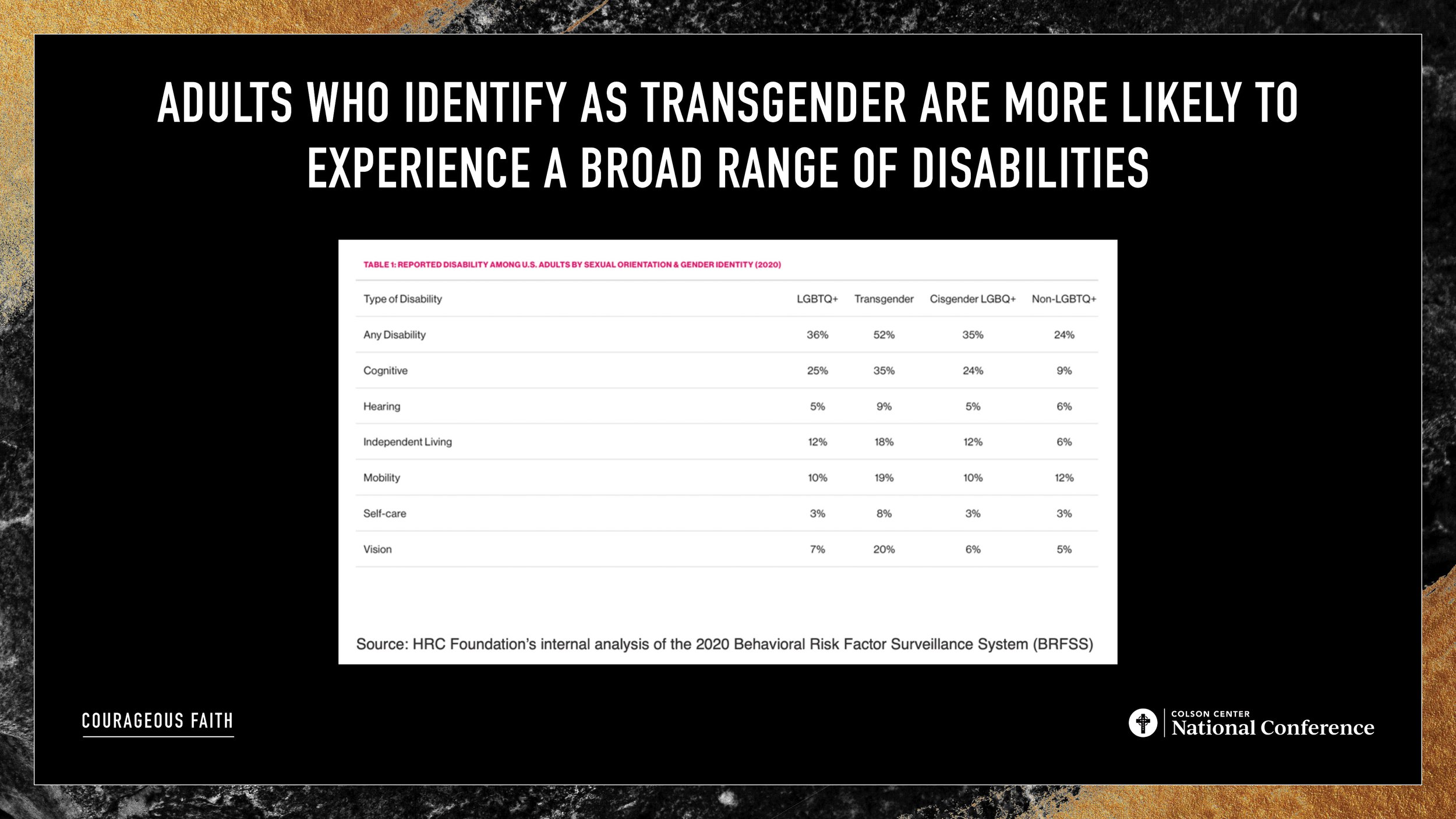
It's not just kids at risk for this gender madness. These are statistics from the Human Rights Campaign. Transgenderism is overrepresented among adults with a broad range of disabilities. Cognitive disabilities, vision or hearing loss, mobility or capacity for self-care and independent living.
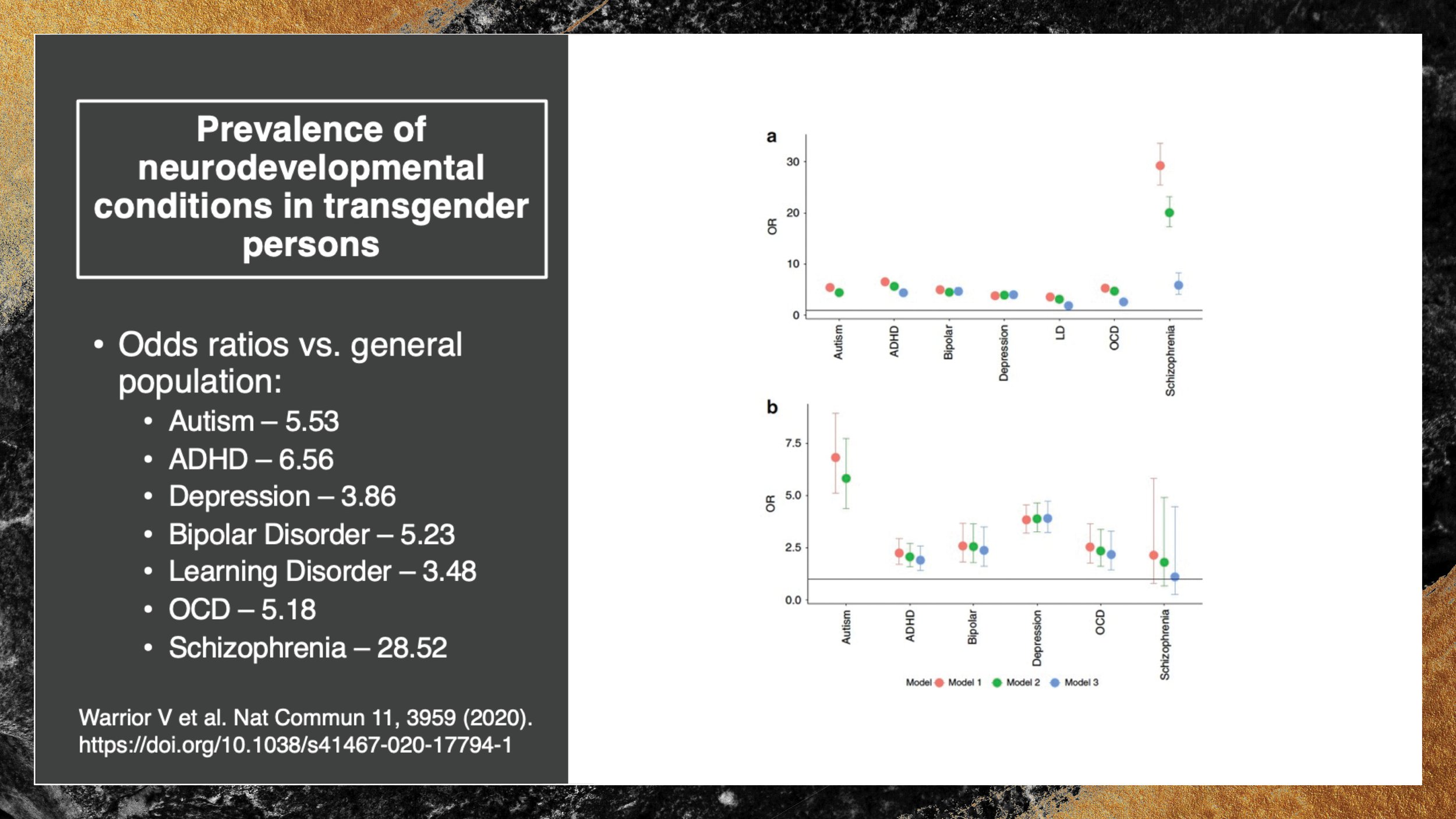
This study from the U.K. illustrates the susceptibility of adults to the transgender ideology. Adults with autism are 5 ½ times more likely than other adults to identify as transgender. Rates are 6 ½ times higher for adults with ADHD, nearly four times higher for adults with depression, five times higher for adults with bipolar disorder or OCD and TWENTY-EIGHT times higher among adults with schizophrenia.
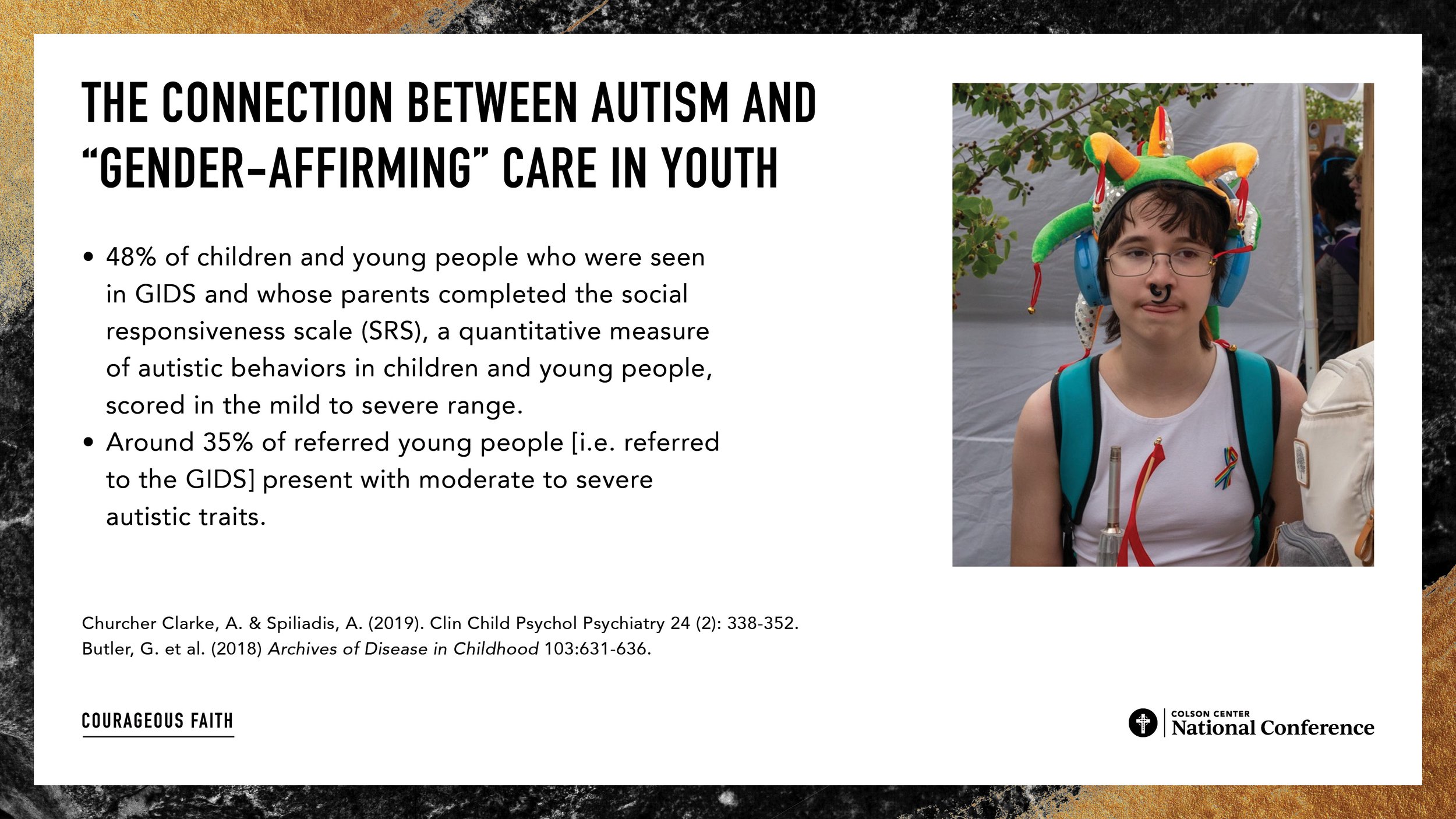
The silence from disability advocates about the high rates of autism among kids treated at gender medicine clinics has been deafening. Before the British Health Service shut down the Tavistock Center - the clinic responsible for treating kids with gender dysphoria from throughout the U.K., nearly 50% of their patients had indications of at least mild autism based upon one screening tool used and 35% of kids receiving puberty blockers or cross-sex hormones were diagnosed with moderate to severe autism.
About five years ago, I was approached about testifying before state legislatures considering action to limit the availability of “gender-affirming” care to children and teens. I had lots of rationalizations for not getting involved…I didn’t consider myself an “expert.” I didn’t need activists coming after my practice, as was the case for an adult psychiatry colleague in my community who has published extensively in professional journals questioning the research cited in support of the treatment. I didn’t want advocacy on this issue to distract from our ministry’s work. But my conscience continued to bother me.
My in-person appointments occur in the homes of the families I serve. Last Spring, I was at the kitchen table of a family I’ve known for a long time with a son is on the high end of the autism spectrum. He’s struggled with social isolation. His parents were thrilled when he found a friend group to eat with at school. Their excitement ended when they discovered his entire circle of friends were girls who thought they were boys. Lunchtime conversations focused on swapping strategies for persuading parents to take them to the gender clinic at the local children’s hospital. I’ll never forget the terror on the mother’s face as the tenacity of his newly acquired identity was on display.
I’d be betraying my profession and my ministry calling by ignoring what my profession is doing to kids. To quote the title of Rod Dreher’s most recent book, each of us needs to choose whether to “live not by lies.” I can’t ignore the lies anymore.
It doesn’t take a lot of courage for an older guy like me to say what I just said. I’m at the end of my career and have relatively little to lose. I’d like to think of myself as having been persecuted when my med school took away some teaching opportunities, but they weren’t paying me enough to consider it persecution. It’s a lot harder for colleagues with student loans and mortgages, working in specialties demanding a connection with a large institution.
What do we do to love our neighbors with disability? We need a two-pronged approach – one addressing the systems and institutions upon which they depend, and the other addressing their need for community – and our need to be in community with them.
We need a “Benedict Option” of sorts within the caring professions in which the remnant who refuse to bend the knee to the spirit of the age can connect with one another, strengthen one another, encourage one another and disciple one another. We need to establish our own societies and institutions to form a next generation of doctors and nurses who recognize their patients with disabilities as image bearers of God. We need to establish support structures to allow physicians and other caregivers to act with integrity before they’ve cultivated great amounts of courage. We need you to buy us some time to build up enough physicians with enough courageous faith to push back against the influences that have hijacked our profession.
This is my daughter Leah, and my son-in-law Max. They’re residents at Mayo Clinic, Leah’s in OB/GYN and Max is in surgery. They’re the future leaders of our healthcare system. How will they, and their peers know how to practice with integrity to their faith if I don’t model what that looks like? I’d encourage each of you to consider how you might model integrity with the truth wherever God has positioned you.

I shared earlier that I’m retiring from clinical practice next year to lead our ministry full-time, but for now, I’m trying to discern whether I might still have role in medicine perhaps as a teacher or mentor to students and younger colleagues. I’d appreciate your prayers that I’ll find a God-honoring role as a physician that doesn’t detract from my ministry calling.
What can we do to love our neighbors with disabilities? Offer them our presence. Spend time with them. I’m convinced far fewer people with chronic illnesses would be seeking physician-assisted suicide if they didn’t have to suffer alone. Get to know the neighbors whose child is picked up by a van on school days. Provide dinner to the person in your office caring for an elderly parent or a child with a disability. Invite them to join you at church for a worship service or some other activity.

Against such things there is no law.
Thanks to John and the Colson Center team for the honor of sharing with you today. Interested in courageously serving families with disabilities? Message me at steve@keyministry.org.

